





 “Contraception, Use It!” That’s a direct quote from Dr. Kieya King at Christie Clinic. Sounds simple enough. So what’s the problem? It’s a question of persistence, a lot of persistence. Most birth control pills are designed to be taken daily. That’s 1,825 pills for 5 years, 9,125 pills over 25 years. And we wonder why people miss! Most people just aren’t that good at the everyday. Ask your local dentist about flossing, and he or she will say the same thing. According to Scott Anderson, D.D.S. from Cosmetic and Family Dentistry, “Most patients who say they floss ‘daily’ still miss occasionally. I’m sure we have some patients who floss every day, but they are undoubtedly the exception. The vast majority of our regular flossers skip a day or two a week.” And so it goes with birth control.
“Contraception, Use It!” That’s a direct quote from Dr. Kieya King at Christie Clinic. Sounds simple enough. So what’s the problem? It’s a question of persistence, a lot of persistence. Most birth control pills are designed to be taken daily. That’s 1,825 pills for 5 years, 9,125 pills over 25 years. And we wonder why people miss! Most people just aren’t that good at the everyday. Ask your local dentist about flossing, and he or she will say the same thing. According to Scott Anderson, D.D.S. from Cosmetic and Family Dentistry, “Most patients who say they floss ‘daily’ still miss occasionally. I’m sure we have some patients who floss every day, but they are undoubtedly the exception. The vast majority of our regular flossers skip a day or two a week.” And so it goes with birth control.
So the dismal facts are that, all these decades after the pill birthday — 50 years strong and going — over half of the pregnancies in the United States are unwanted. And yes those skipped days are a big offender, with failure rates for the pill being as high as 8%, especially in teens who seem to forget pills as much as 67% of the time, and have failure rates as high as 12–15%.
Though a branded pill does cost more than condoms, they are fairly affordable for many. At McKinley Health Center they range from $5 to $9 per month.
Free gift with purchase
The oral contraceptive pill is truly the gift that keeps on giving. You may think you’ve only gotten protection from pregnancy, but in reality there are a couple of dozen significant non-contraceptive side benefits as well.
Non-contraceptive benefits of the pill include a reduction in:
• Menstrual cramps or pain (dysmenorrhea) and endometriosis prevention
• Prevention of Ovarian Cysts and Ovarian cancer
• Cancer of the endometrium (uterine lining)
• Improvement or treatment of Acne
• Reduced Iron-deficiency anemia (a low blood count due to low iron levels)
Safe use of the pill, new medical guidelines
Medical eligibility for birth control use, with versions in many languages (including both African and Brazilian Portuguese) can be found at the World Health Organization (WHO) website.
And if you prefer your documents to only list contraceptive methods that we can actually get in the US, turn to the CDC document. Our tax dollars actually at work!
A lot of the safety of oral contraception has to do with the fact that pill doses of estrogen have dropped from the 150 mcg of estrogen in the days of yore to the 20-35 mcg range of most pills today, and progesterone dose has been cut more than ten-fold. Dosing does not just include the number of milligrams either; you have to know what is in your pill. For example, a pill with mestranol is much weaker than the ethinyl estradiol pill because mestranol is actually converted to ethinyl estradiol in the blood stream. And we now have Natazia, a pill with the estrogen estradiol valerate, which is converted to the bioidentical estradiol in our blood stream.
Should you worry about taking oral contraception if you’re overweight?
Contrary to the earlier studies that reported failure rates up to 40% higher in women who are obese, Carolyn Westoff and researchers at Columbia University have taken a new look at oral contraception hormone levels in women who are obese, and found that the levels of hormone are just fine.
Dr. James Trussell, the director of the Office of Population Research at Princeton University in New Jersey, still cautions pill use in obese women: “I would say that the pill is still not going to be the front line, the top tier contraception for obese women.” Trussell goes on to suggest that in “methods with a lower risk of failure due to human error, like the IUD, hormonal implants, or vasectomy for the male partner, would likely be a better choice.” Moreover, in a recent Reuters article we have a shout out for my favorite belt and suspenders kind of treatment: “If a woman really doesn’t want to become pregnant I would suggest combining oral contraceptives with a barrier method,” said one of the consultants. So if you are looking for something that is a bit hands-off, give some thought to getting the Implanon rod that lasts for three years when placed under the skin of your arm, and is practically as skinny as the lead in a pencil.
Special considerations: Athletic performance, mate selection
Pills are an effective form of contraception, and healthy for your body. But now and then some interesting facts pop up in the literature about what else the pill affects. We all know that the pill can cause a bit of extra bloat, leading you to not look as great in those tennis whites, but it can also reduce your male hormone blood levels. Not great if you put a premium on whacking that tennis ball hard, but great if you don’t want to have a mustache in the tournament picture gallery! So benefits become a risk and risks become benefits, or a better way to say this, is that each woman has her own risk benefit ratio, and you want to be sure yours is favorable.
Another odd fact: have you ever thought about how you would react to odors while on the pill? No one has probably ever thought that their particular olfactory senses would change, but taking oral contraception could possibly change your smell perception. An recent interesting discovery: “The use of the pill by women, by changing her mate preferences, might induce women to mate with otherwise less-preferred partners, which might have important consequences for mate choice and reproductive outcomes,” said Alexandra Alvergne, lead author of a study appearing in the October issue of Trends in Ecology & Evolution.
IUDs
And for those forgetful gals, you just need behavior-free contraception, sort of the ever-ready approach. IUDs are excellent in that they just sit in the uterus. You don’t have to think about whether they are working; you just use them. Barriers to use of long-term methods like the ParaGard IUD or the Mirena IUS, include worries about the cost, as well as fear of side effects. And the the Mirena IUD can have sexual side effects, as reported in the blog post. Find the lively discussion here.
For over half of all women in China and in Europe the most popular long term contraceptive is the IUD. But market penetration (pun intended) is just not as good in the US, with only 2% of women choosing this method (though the numbers are on the rise). Contraceptive efficacy with the IUD/IUS is excellent, and oddly, as popular as these devices actually are in the Orient, the Chinese still have a bit of a method failure problem with IUDs, like the Mahua’ ring: a seven sized ring IUD manufactured in Tianjin, which is designed for very long term use.
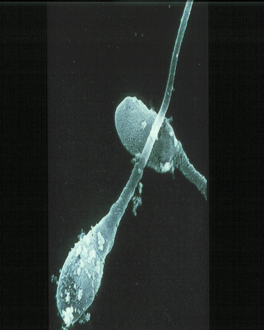
Some maintenance is required
Always get screened for STDs. We transmit bacteria in many creative ways. The photo at the right shows some hitching to the fallopian tubes on the backs of sperm.
Is hormone-free your interest?
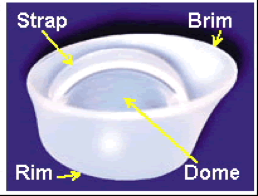
Barrier methods have some new twists on old concepts, such as the Lea’s Shield, which is available at some Planned Parenthoods. Or you can just order one up with a handy form that you can have your doc sign.
Figure 3. Lea’s Shield Barrier Method, from Contraceptiononline.com (pdf)
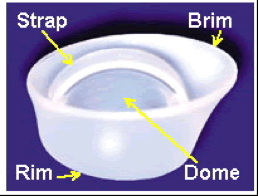
There is also the FemCap. Just be sure to get your correct size, available in small, medium, or large. The fit of FemCaps, rim towards the cervix, form.
Have you thought of trying Bellagio? It’s not in Vegas. It’s not a new sexual technique. It’s an old, and quite presentable contraception topic. The Consensus Conference on Lactational Infertility was held in August 1988, in the town of Bellagio, Italy on the shores of Lake Como, and has to do with what we have come to call LAM: contracepting through breast feeding, or lactational amenorrhea. It is a great concept, and yet may not provide the full contraceptive efficacy that you want, especially if you are an American woman who skips those night feedings to get in a full three 3-4 hours of sleep instead of continuing to feed every two hours. And just because you don’t conceive, the contraceptive effect may not extend to complete suppression of all ovarian follicular activity. We have discovered this due to ultrasound technology and the widespread use of getting ultrasounds with gynecologic complaints. So if you want to know whether it’s really working or not, there are a few tests that can help: progesterone levels is a test that can detect signs of ovulation; checking your cervical mucus or your urine for ovulation is another way.
Today’s diaphragm is not your mother’s diaphragm. The new latex-free alternative from Milex may be popular enough to bring back memories of the diaphragm scene in Goodbye, Columbus. For more information check CooperSurgical.com (pdf).
Alternatives: Catch it, Patch it or SPERMs?
Catch that ovulation before it happens. The EllaOne, also called the MAP (Morning after pill), which contains ulipristal was just approved as an emergency contraceptive pill (ECP) that will be effective up to about five days after unprotected intercourse. It works on the progesterone receptor. In actuality it has some properties like progesterone, but also some anti-progesterone properties, or a “selective progesterone receptor modulator,” fondly called a SPERM–more accurately a SPRM–by those in the know. Look for it at your pharmacy by November, but also remember this: unlike Plan B, everyone will will need a prescription, not just those under 18. Prescriptions over the phone are available at Women’s Health Practice.
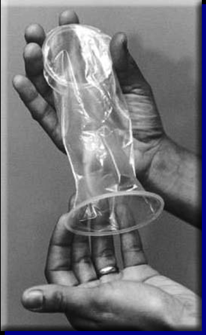
Also available are a variety of new devices, from creative male condoms to the nitrile made (non-latex) female condom.
Patch it? Patches for contraception have been available before. But only if you are interested in the patch, and interested in participating in a study (although enrollment may close soon). Go to the Website of the New Choice Study. You can get there through Craig’s List or just go to their website.
Kill those sperm. The approach to microbicides has always been to kill off sperm (with their piggy-backing bacteria) in the vagina with a sort of disinfectant approach. The newest approach is to put the anti-HIV treatments right into the vagina. A recent African research study, released in July, states that CAPRISA gel antiretroviral (ARV) tenofovir reduced sexual transmission of HIV infection by 39%, and was 51% effective in preventing genital herpes infection.
In conclusion, let me repeat: Contraception: just use it. For if not: pregnancy. And for that you should be prepared. More on that in another article.
Editors Note: Suzanne Trupin is currently a paid contraceptive consultant for: Teva and Ferring Pharmaceuticals and has been a consultant for Bayer HealthCare and Pfizer Pharmaceuticals in the past.